


What is vitamin D?
Vitamin D, or the “sunshine vitamin,” is an interesting fat-soluble vitamin because it’s the only vitamin our bodies can make from the sun.
In fact, the sun is our main source of vitamin D, providing anywhere from 50-90 percent of our vitamin D needs (1).
Like vitamins A and K, vitamin D has two forms, D2 (ergocalciferol) and D3 (cholecalciferol), both of which are found in small amounts in food: D2 in plant foods and D3 in animal foods. Processed foods, such as cereals, are often fortified with vitamin D (though, like any other fortified food, this is not the ideal way to obtain it).
Vitamin D is one of the most studied vitamins when it comes to pregnancy, as it is related to so many important functions to keep you and your baby healthy.
Vitamin D deficiency is common during pregnancy; over 80% in the second trimester, according to a 2026 meta-analysis (2). However, vitamin D deficiency is a problem worldwide. Most people in the US consume less than the recommended amounts of vitamin D (1).
This is due to multiple dietary, lifestyle, and physiological factors, which we will examine in more detail below.
Vitamin D & Fertility
Vitamin D status may influence fertility outcomes.
Overall, studies suggest that having sufficient vitamin D before conception (often defined as 25(OH)D ≥30 ng/mL / ≥75 nmol/L) is associated with slightly higher pregnancy and live birth rates, especially among people who start out deficient. However, results aren’t perfectly consistent across all populations.
What the evidence suggests
- Natural conception: In prospective data, women with sufficient preconception vitamin D had a higher likelihood of clinical pregnancy and live birth (approximately 10–15% higher live birth likelihood in some cohorts) and, in some studies, a lower risk of pregnancy loss (1, 2, 3).
- Infertility treatment/ART: Vitamin D status may be relevant for both partners. A couple-based analysis found a higher likelihood of live birth when the female partner was sufficient, and outcomes were strongest when both partners were non-deficient; however, IVF-specific meta-analyses have reported mixed or non-significant associations after sensitivity analyses (4, 5, 6).
- Supplementation: In infertile patients, vitamin D supplementation has been associated with improved clinical pregnancy rates, with the greatest benefit observed in individuals who are vitamin D–deficient at baseline (7).
Vitamin D & Pregnancy
Vitamin D supports key processes during pregnancy for both the parent and the baby. Low vitamin D status has been associated with a higher risk of complications, though not all studies find the same strength of effect.
Pregnancy outcomes
Vitamin D deficiency has been linked to gestational diabetes, preeclampsia, first-trimester miscarriage, and gallbladder issues.
Vitamin D plays a role in glucose metabolism, but research on whether low vitamin D causes gestational diabetes is mixed (3). Still, vitamin D levels are often lower in people with GD, so it’s worth checking. Evidence on preeclampsia is also mixed, but many studies suggest that levels above 30 ng/mL are associated with a lower risk, and some data suggest that supplementation later in pregnancy may be more effective than early supplementation (4, 5, 6).
If levels are low, supplementation can be useful, but it works best alongside the root habits that support vitamin D status—sun exposure, vitamin D-rich foods, and addressing absorption/metabolism issues.
Impact on baby
The baby relies entirely on the mother for vitamin D in pregnancy.
Maternal deficiency has been associated with a higher risk of certain childhood outcomes (including asthma, neurodevelopmental concerns, and autoimmune conditions) and may affect fetal bone development (research is still emerging) (4, 7). Low vitamin D status during pregnancy has also been linked to low birth weight and an increased risk of rickets (4).
Vitamin D & Postpartum
Vitamin D is essential during the postpartum period and while breastfeeding for maternal health and baby development.
It’s needed for a baby’s bone health, immune function, and the prevention of rickets (62). Rickets is a softening and weakening of the bones in children caused by prolonged vitamin D deficiency, which remains a risk after the baby is born (62).
Vitamin D also supports immune and bone health in postpartum and nursing mothers. Additionally, it’s essential for mood and mental well-being. Deficiency of vitamin D may be a risk factor for postpartum depression (63).
Vitamin D & Breastfeeding
It’s widely recommended that mothers who exclusively breastfeed provide their infants with vitamin D, but have we ever stopped to consider why breast milk might be lower in vitamin D in the first place?
If you are not getting enough vitamin D from sunlight and food, you cannot transfer enough vitamin D through breast milk to your baby, even if your levels are normal (8).
This is because adequate vitamin D levels in the blood do not transfer through breast milk (8). However, vitamin D from sunlight, food, and supplements will transfer over to your baby (8)!
One study found that breastfeeding women who took 6400 IU of vitamin D per day had optimal vitamin D levels in their blood and transferred sufficient vitamin D through their breast milk to meet their baby’s needs without requiring additional supplementation (8).
So, if you’re planning to breastfeed, it’s a good idea to start planning how you will supply your little one with enough vitamin D, ideally through a combination of food, sunlight, and a vitamin D supplement to ensure their needs are met.
Vitamin D needs at every stage
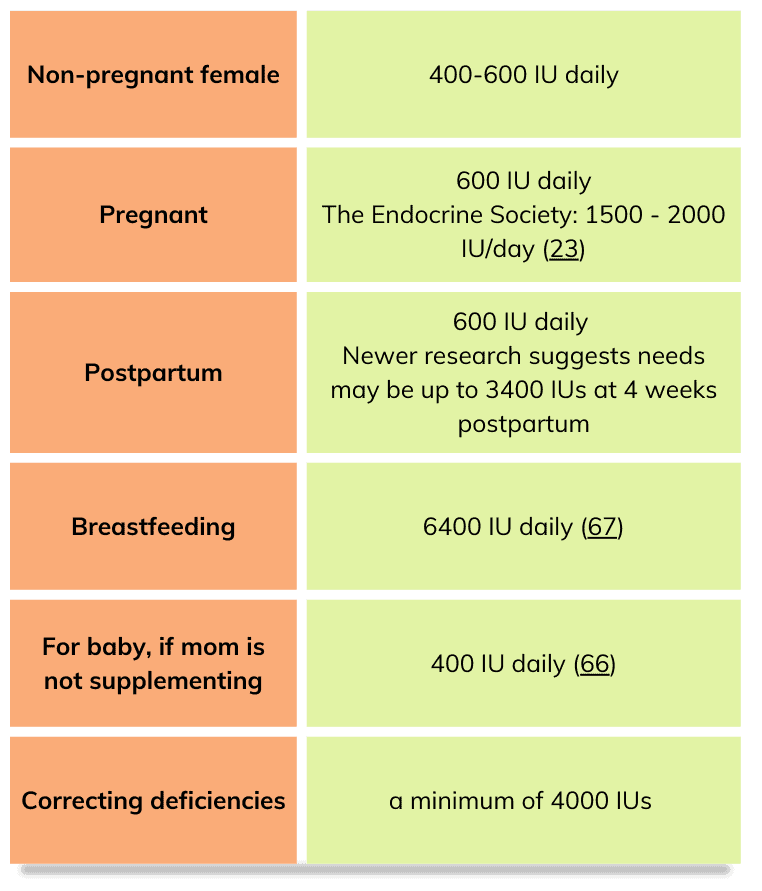
Research is inconclusive about the exact amount of vitamin D needed at any stage, but most people will need to supplement with vitamin D. Review the prenatal vitamin note to find a prenatal vitamin with more vitamin D than 400-600 IUs.
Vitamin D deficiency
Vitamin D deficiency is a global problem, with many people not getting sufficient sunlight exposure, especially those who work all day indoors and never get daytime sunlight.
Many countries have different cut-off points for ‘adequate’ vitamin D levels, making it difficult to quantify precisely how many people experience vitamin D deficiency (4).
Risk factors for vitamin D deficiency:
- Living North of the line drawn from Long Beach, CA, to Atlanta, GA
- Living in an area with more air pollution
- Dark skin
- Obesity (4)
- Wearing sunscreen (at all times) when outdoors
- Wearing long sleeves and pants outdoors
- Vegetarian/vegan
- Little time spent outdoors, especially at midday
- Lactose intolerance (9)
- Smoking (4)
Limited sun exposure, sunscreen, and vitamin D deficiency
A major risk factor for vitamin D deficiency is limiting sun exposure or always wearing sunscreen when outdoors.
Fear of skin damage has led to the overuse of high-factor sunscreen. It is important to be careful about skin damage, and everyone’s limits will be different, but your skin needs access to midday sun a few times a week to synthesize vitamin D.
And it turns out the sun isn’t all to blame for sun damage and skin cancer— your diet is a contributor, too!
The link between vegetable oils and skin cancer
Did you know that another sneaky culprit can greatly increase your risk of skin damage and skin cancer (along with countless other diseases and issues)?
Research shows associations between linoleic acids (found in vegetable oils such as canola, corn, and soy) and an increased risk of skin cancer (10). While correlation doesn’t prove causation, studies also show us that reducing seed oils can “dramatically reduce the risk of ultraviolet (UV) induced sunburn,” with “susceptibility to UV radiation damage of the skin is directly influenced by the amount of LA (linoleic acid) in the diet” (10)!
This makes sense when we consider how seed oils can become rancid; similarly, they can cause DNA damage throughout the body, including the skin, especially when exposed to heat, such as sunlight, leading to cancer (11).
Keep in mind: while linoleic acids are the most prone to oxidation of all oils, the more unsaturated a fat is, the more prone it is to oxidation, while naturally saturated fats (i.e., animal fats and coconut oil) do not have the same damaging and dangerous effect in the body (12).
Learn more about which oils to choose and which to limit during pregnancy here!
How to safely get vitamin D from the sun
Maximize more D intake in less time
The best time to get vitamin D from the sun is at its highest point in the sky, which is midday (especially during the summer months), when the UVB rays responsible for vitamin D production are most intense (13, 14).
Spend 15-30 minutes in the sun.
Fifteen minutes in the hot summertime sun and at least 30 minutes in the wintertime when the rays are less intense (15, 16). If you have darker skin (either you’re someone who gets a tan easily or you were born with darker skin), you will need more time in the sun to get enough since having more melanin blocks the sun’s UVB rays, which is one reason why those with darker skin are at a higher risk of vitamin D deficiency than those with fair skin (17).
The good news is that by maximizing your time in the sun when UVB rays are at their peak, you can get your vitamin D without increasing your risk of skin damage or melanoma (14). You can even use the D-minder app to help you make sure you’re getting enough vitamin D based on your skin and location.
If you are planning to spend more time in the sun (>30 minutes), stay in the shade, cover up with UV-protective clothing and a hat, or wear a mineral-based, paraben-free sunscreen!
Increase your antioxidant intake.
In addition to reducing your risk of sun damage by limiting your linoleic acid intake as much as possible, you can increase your intake of astaxanthin, which research has found to have anti-aging and anti-cancer effects by reducing the effects of harmful UV rays (18, 19). Foods high in astaxanthin include salmon, algae, shrimp, lobster, crabs, and other seafood.
Vitamins A, C, and E also act as sun and skin-protective antioxidants as well, so load up on your citrus and whole food fats, like butter, nuts, avocados, and full-fat dairy (20).
 Vitamin D-rich foods
Vitamin D-rich foods
As noted, the primary source of vitamin D is sunlight, and it is not found in many foods. The best dietary sources are oily fish like trout and salmon.
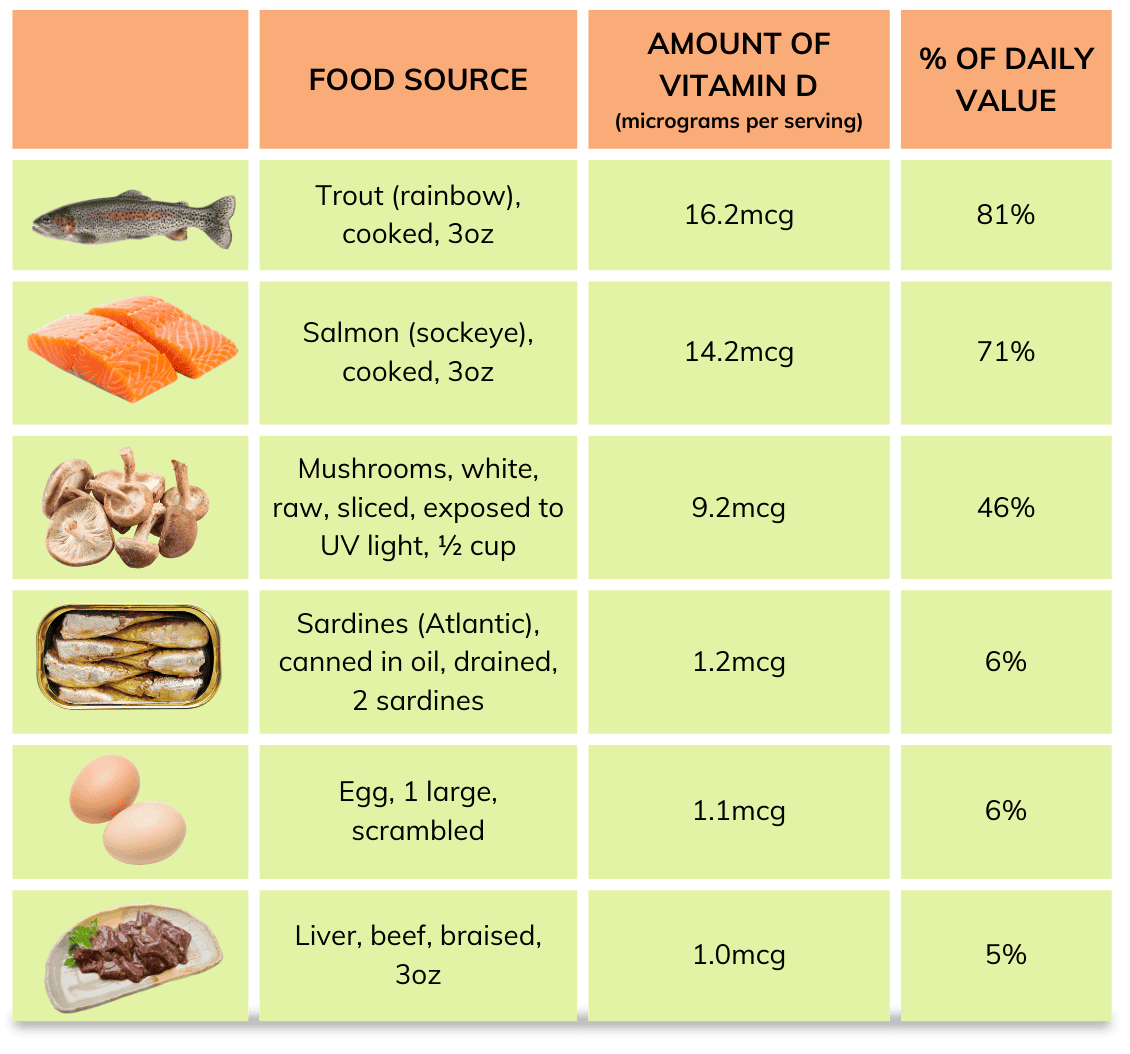
(Table adapted from National Institutes of Health 2021)
Vitamin D testing
By testing your vitamin D levels (25-hydroxy vitamin D, or 25-OH vitamin D), you can fine-tune how much you need to supplement, working with your doctor and registered dietitian. I highly recommend this.
While you will see a level of 30 ng/ml (75 nmol/l) is sufficient, research indicates pregnant people should be closer to 50 ng/ml (125 nmol/l) (24).
You can also order an at-home vitamin D test kit.
Do I need to supplement with vitamin D?
You’ve probably already gathered from above – yes, but there is a bit more to it than that.
Find a prenatal vitamin that contains vitamin D3 (cholecalciferol). Although many of you reading this will need more than even what the Endocrine Society recommends (1500 – 2000 IU/day), taking a prenatal vitamin with at least 1000 IU is strongly recommended.
A double-blind, randomized clinical trial found that 4,000 IU/day of vitamin D supplementation was safe and the most effective in achieving sufficient vitamin D levels in all women, regardless of race or geography (25).
If you can, get your levels tested before and during each trimester of your pregnancy, including the fourth trimester.
The good news is that vitamin D supplements are relatively cheap! If your prenatal vitamin doesn’t contain vitamin K2 or phylloquinone, then it is recommended that you find a D3 supplement with K2. See some recommendations next.
Vitamin D supplement recommendations
- Thorne’s Vitamin D/K2 drops (2 drops = 1000 IUs)
- Seeking Health Vitamin D3 + K2 capsules (5000 IUs) (code: RyannK)
- Seeking Health Vitamin D3 capsules (5000 IUs) (code: RyannK)
- Thorne’s Vitamin D3 capsules (5000 IUs)
- Pure Encapsulations capsule (1000 IUs)
- Needed has a vitamin D3 + K2 capsule (2000 IUs)
- Nordic Naturals lemon cod liver oil (1 teaspoon = 1000 IUs, also contains omega-3s!)

Help! My vitamin D is still low despite supplementation. What could be the problem?
It can be frustrating if you’ve had chronically low vitamin D levels despite supplementing. But often, the key to low vitamin D isn’t just adding more vitamin D; it’s addressing the contributing factors that led to the low vitamin D in the first place.
Other potential causes of low vitamin D
Low magnesium
Magnesium is needed to move vitamin D around in the blood and to activate vitamin D or convert it from its storage form to active form, and this can only happen when you have enough magnesium (26, 27). Magnesium deficiency can also reduce active vitamin D (1,25-dihydroxyvitamin D) levels and impair parathyroid hormone response (26).
If you’re trying to address a vitamin D deficiency without also making sure your magnesium levels are adequate. With over half of the population in the US not getting enough magnesium each day and with magnesium needs being higher during pregnancy, it’s a good idea to pay more attention to your magnesium intake during pregnancy and get your levels checked in an RBC magnesium test and/or HTMA to determine if you already have a magnesium deficiency contributing to vitamin D deficiency (28, 29, 30).
Having higher body fat
Since vitamin D is fat-soluble, people with higher body fat will store it in fat cells, leading to less circulating in the blood. People with obesity need higher vitamin D intake to maintain adequate levels and/or correct a deficiency (31).
So, being obese reduces your body’s ability to convert vitamin D and circulate it, and reduces the effectiveness (32, 33). If obesity is a risk factor for you, this means you have a higher chance than average of being vitamin D deficient and responding poorly to supplementation, which means you will need a targeted protocol for assessing and ensuring your levels are adequate during pregnancy.
Chronic infections and inflammation
Bacterial infections may cause dysregulated vitamin D metabolism (34). Chronic infections might include chronic Lyme disease, mycotoxin-related illness, and Epstein-Barr virus, which has been found to inactivate vitamin D receptors (35, 36). It’s best to work with a functional practitioner to address root issues and treatments if you know or suspect you have one of these or another.
Your genetics
Some studies show that genetic variants, including those in VDR, CYP2R1, CYP27B1, and GC, may affect the benefit of vitamin D supplementation for each individual (37, 38, 39).
Not eating enough animal foods and animal fats
Micronutrients needed for vitamin D synthesis and use in the body include cholesterol, magnesium, vitamin A, and vitamin K (40, 41). These are all found in animal foods, so if you have a low intake of foods high in these nutrients, your vitamin D metabolism will be impaired. Review our vegetarian note here for more information.
Poor gut health
An imbalanced gut microbiome is associated with lower vitamin D levels, but increasing beneficial bacteria has been shown to raise vitamin D levels (42). Gut health is a key foundation for overall health, fertility, and pregnancy, and if your gut microbiome is out of balance, your vitamin D levels will likely remain out of balance as well.
For more on how to support gut health during pregnancy, read on here.
Conditions that affect nutrient absorption, such as celiac disease, Crohn’s disease, and Cystic Fibrosis, all reduce your body’s ability to absorb vitamin D (43).
Poor bile flow
Poor bile flow reduces your ability to absorb fat-soluble vitamins (vitamins A, D, E, and K) since bile is responsible for breaking down fat, but you can increase bile and support bile flow by supplementing with bile salts, which have been found to increase vitamin D levels (42). You can also support increased bile flow by eating plenty of fats (cholesterol, especially), beets, and glutamine-rich animal foods, such as meats, seafood, and dairy, as well as choline from eggs and liver (44, 45).
High glyphosate exposure
People can be exposed to glyphosate through diet, skin contact, and inhalation of airborne particles. Fruits, fruit juices, vegetables, and cereals all contain this herbicide (46). Glyphosate reduces vitamin D by reducing both the CYP27A1 gene and other minerals needed for vitamin D metabolism (47, 48, 49). Buy organic produce if possible, especially the dirty dozen.
Hyperparathyroidism
Hyperparathyroidism is caused by abnormal parathyroid gland growth and elevated parathyroid hormone secretion, which, among many other symptoms, can lead to low vitamin D levels. It is most common in women over 60 years old, but it can also occur in younger people (especially women) (50).
Some or many of these might be factors in your own situation, and it’s ideal to work with a practitioner who can dive into your health history to find what could be causing your deficiency rather than just trying to increase supplementation of vitamin D alone.
Other lab values to assess when addressing vitamin D include:
- Active D and storage D: 25-hydroxy vitamin D (vitamin D stores, most commonly used), and if suspected high active vitamin D levels, 1,25-dihydroxy vitamin D (active form, less commonly used). Usually, only storage vitamin D is tested, but it is possible that you may have low-storage vitamin D and high-active vitamin D, especially if you’re supplementing vitamin D and have trouble converting vitamin D.
- Ionized Calcium: unbound calcium that is not bound to protein and is the body’s most accurate measure of calcium (51).
- RBC magnesium: a more accurate indicator of magnesium levels in the cells (only 1 percent of magnesium is actually in the blood) (29). An HTMA (hair test) can also provide good insight into intracellular magnesium levels.
- Parathyroid hormone: Vitamin D deficiency is common in hyperparathyroidism (52). High PTH levels can lead to high 1,25(OH)2D, low bone mineral density, increased risk of fractures, and osteoporosis, and supplementing with vitamin D often leads to low or suppressed PTH (53, 54).
Start here with increasing vitamin D levels
Like most nutrients, vitamin D works best with consistency. So, do your best to consume vitamin D–rich foods regularly (fatty fish, egg yolks, and full-fat dairy if you tolerate it).
Then use these three levers to help your body absorb and use vitamin D more effectively:
- Optimize magnesium levels : Prioritize magnesium-rich foods (pumpkin/chia seeds, almonds/cashews/peanuts, spinach, beans, edamame). If needed, add magnesium via a supplement (multi-form options like Smidge), topical magnesium (lotion/deodorant), Epsom salt baths, and/or magnesium powder in your daily mineral mocktail
- Eat more animal foods and fats: Vitamin D metabolism relies on nutrients found mostly in animal foods—especially cholesterol, vitamin A, and vitamin K2 (40, 41). Focus on egg yolks, full-fat dairy/cheese, grass-fed beef, and (if you tolerate it) small amounts of liver/organ meats; include fermented foods for K2 like miso, sauerkraut, or natto. Cholesterol matters, too, because vitamin D made from sunlight is synthesized from cholesterol (56).
- Go outside mid-day. : Start by going outside mid-day without sunscreen or sleeves (if it isn’t winter).
Can you get too much vitamin D?
Yes!
Too much vitamin D is toxic, another reason to test your levels before reaching for really high-level supplements.
When vitamin D is truly excessive, it can:
- Raise calcium too high (hypercalcemia) in both mom and baby (4)
- Cause symptoms like vomiting, muscle weakness, dehydration, and kidney stones (57)
- Increase risk of soft tissue calcification (potentially via potassium wasting) (58)
- Deplete magnesium, which vitamin D relies on for metabolism (59)
That said, studies using 4,000–5,000 IU/day have not shown hypercalcemia or tissue calcification, but vitamin D works best (and safest) when you’re also getting adequate supportive minerals that help your body utilize it (60, 61).
Can you get too much sun?
Excessive sun exposure won’t lead to toxic levels of vitamin D, but it definitely isn’t good for your skin. It is possible that frequent tanning beds can lead to toxic vitamin D levels, but they are an all-around bad idea anyway, so best to avoid them.
Written by: Claire Gilmore, MSCN, CNS, LDN, and Ryann Kipping, MPH, RDN, LDN